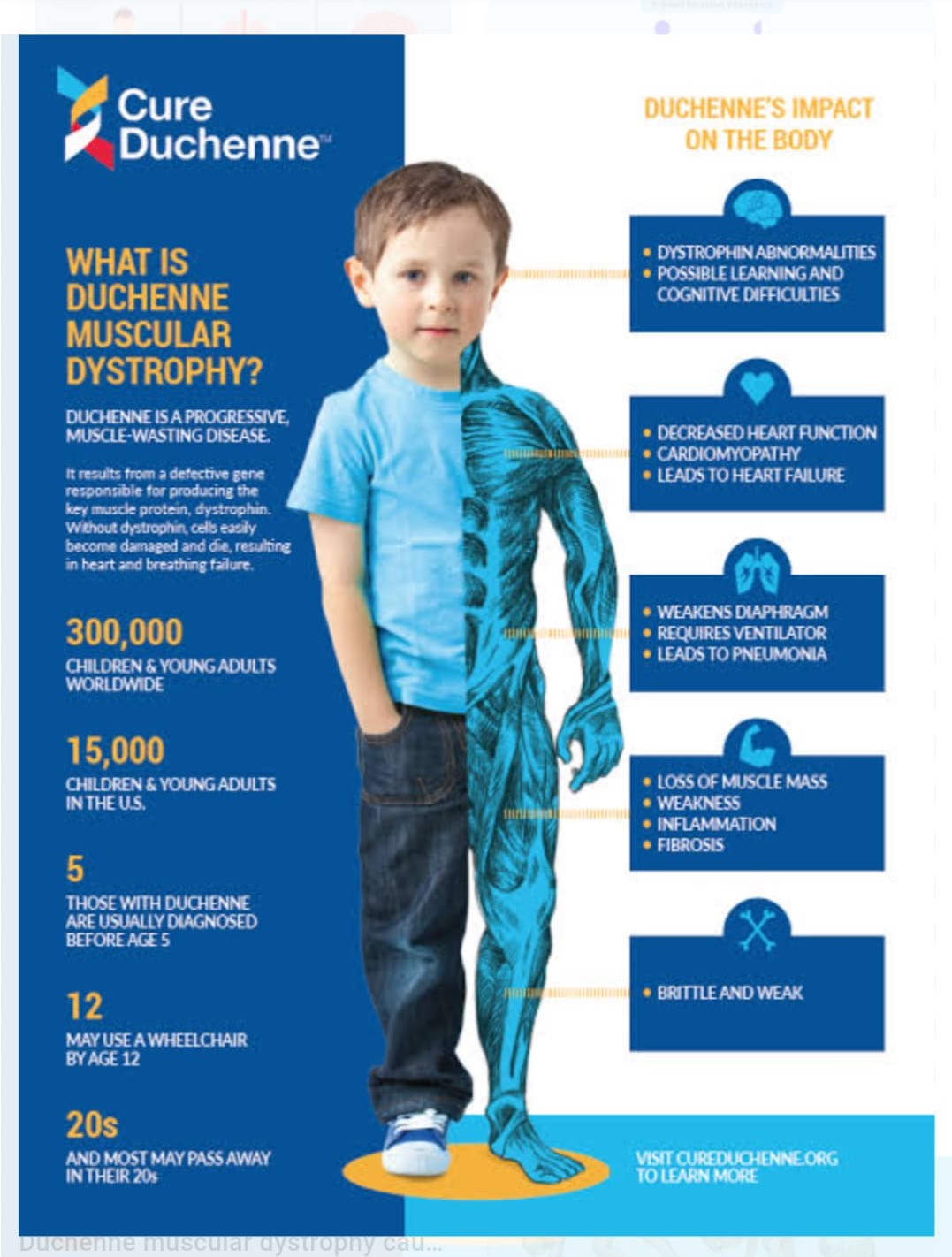
Duchenne Muscular Dystrophy
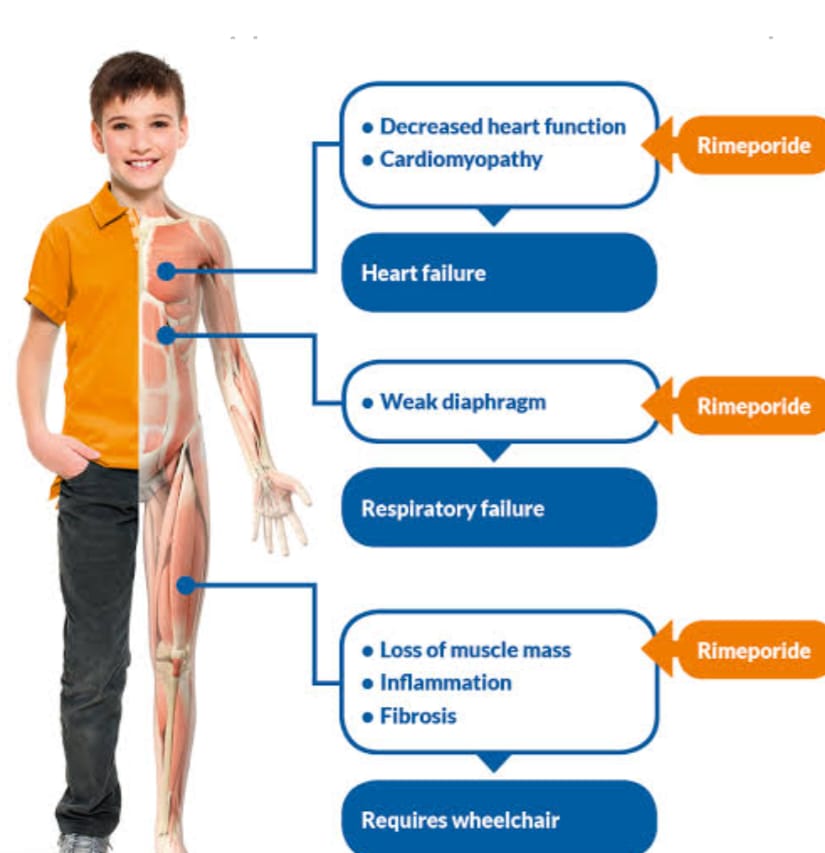
Duchenne muscular dystrophy (DMD) is a severe recessive X-linked form of muscular dystrophy characterized by rapid progression of muscle degeneration, eventually leading to loss of ambulation and death. This affliction affects one in 3500 males, making it the most prevalent of muscular dystrophies. In general, only males are afflicted, though females can be carriers.. This type of muscular dystrophy is most common and most severe. This type affects the pelvic girdle and then moves to the shoulder girdle.
Symptoms usually appear in male children before age 5 and may be visible in early infancy. Progressive proximal muscle weakness of the legs and pelvis associated with a loss of muscle mass is observed first. Eventually this weakness spreads to the arms, neck, and other areas. Early signs may include pseudohypertrophy (enlargement of calf and deltoid muscles), low endurance, and difficulties in standing unaided or inability to ascend staircases. As the condition progresses, muscle tissue experiences wasting and is eventually replaced by fat and fibrotic tissue (fibrosis). By age 10, braces may be required to aid in walking but most patients are wheelchair dependent by age 12. Later symptoms may include abnormal bone development that lead to skeletal deformities, including curvature of the spine. Due to progressive deterioration of muscle, loss of movement occurs eventually leading to paralysis. Intellectual impairment may or may not be present but if present, does not progressively worse as the child ages. The average life expectancy for patients afflicted with DMD varies from late teens to early to mid 20s. There have been reports of a few DMD patients surviving to the age of 40, but this is extremely rare.
Symptoms:-
Awkward manner of walking, stepping, or running. (patients tend to walk on their forefeet, because of an increased calf tonus. Also, toe walking is a compensatory adaptation to knee extensor weakness.)
Frequent falls
Fatigue
Difficulty with motor skills (running, hopping, jumping)
Increased Lumbar lordosis, leading to shortening of the hip-flexor muscles. This has an effect on overall posture and a manner of walking, stepping, or running.
Muscle contractures of Achilles tendon and hamstrings impair functionality because the muscle fibers shorten and fibrosis occurs in connective tissue
Progressive difficulty walking
Muscle fiber deformities
Pseudo hypertrophy (enlarging) of tongue and calf muscles. The enlarged muscle tissue is eventually replaced by fat and connective tissue, hence the term pseudo hypertrophy.
Higher risk of behavior and learning difficulties, due to adjustment problems and muscular fatigue.
Eventual loss of ability to walk (usually by the age of 12) Skeletal deformities (including scoliosis in some cases)
Signs and tests:-
A positive Gowers` sign reflects the more severe impairment of the lower extremities muscles. The child helps himself to get up with upper extremities: first by rising to stand on his arms and knees, and then "walking" his hands up his legs to stand upright.
Affected children usually tire more easily and have less overall strength than their peers.
Creatine kinase (CPK-MM) levels in the bloodstream are extremely high.
An electromyography (EMG) shows that weakness is caused by destruction of muscle tissue rather than by damage to nerves. Genetic testing can reveal genetic errors in the Xp21 gene. A muscle biopsy (immunohistochemistry or immunoblotting) or genetic test (blood test) confirms the absence of dystrophin, although improvements in genetic testing often make this unnecessary.
EIGHT STAGES OF DUCHENNE MUSCULAR DYSTROPHY:
1. Ambulates with mild waddling gait and lordosis. Climbs stairs and curbs without assistance.
2. Ambulates with moderate waddling gait and lordosis. Needs support to climb stairs and curbs.
3. Ambulates with moderately severe waddling gait and lordosis. Cannot climb stairs or curbs.
4. Ambulates with severe waddling gait and lordosis. Unable to rise from a standard height chair.
5. Wheelchair independence. Sits erect and can roll chair and perform all activities of daily living (ADL) and wheelchair activities without assistance. 6. Wheelchair with dependence. Needs assistance when performing ADL and wheelchair activities
7. Wheelchair with dependence. Sits erect only with support. Able to do minimal ADL.
8. Bed patient. Needs maximum assistance for ADL.
Treatment:-
There is no known cure for Duchenne muscular dystrophy, although homoeopathic medicine is showing promising vectors that may replace damaged muscle tissue. Treatment is generally aimed at controlling the onset of symptoms to maximize the quality of life, prevent further detoriation leading to gradual improvement in health status of patients.
One can notice symptomatic improvement within 3-4 months of treatment. Duration of treatment varies with the severity of disease.we have over 6000 patients of all types of muscular dystrophy from all over the world. we have documented up to 80% improvement in our patients.